
Through this blog I have tried to highlight the problems of out-of-pocket expenditure (OOP) and catastrophic health expenditure (CHE) several times. The process is simple- inadequate public spending on health leads to poor health infrastructure and compromised quality of care which forces people to go to private hospitals and care providers who due to lack of a regulatory mechanism charge heavy sums of money, thus leading to catastrophic health expenditure.
Also read- Every year 5 crore Indians are pushed into poverty due to health expenditure
India ranks 6th in out-of-pocket expenditure
India’s per capita General Government Health Expenditure is $ 23
Prof Anirudh Krishna of Duke University calls this the ‘Health Poverty Trap‘ where a household which would have gained some social mobility would eventually fall back into poverty because of an adverse health episode of a family member.
According to a new study published in the BMJ journal every year nearly 55 million Indians are pushed into poverty due to CHE. Most of this health induced poverty is due to massive expenditure on medicines.
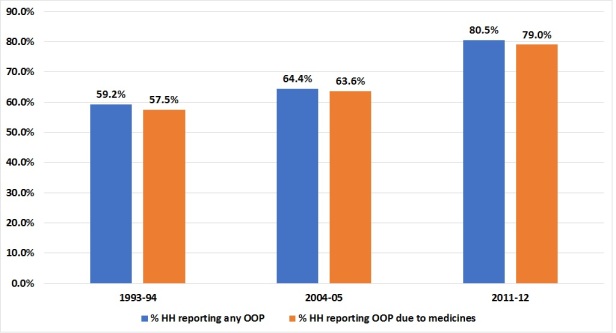
From 1993-94 to 2011-12, the percentage of households that have suffered OOP has gone up from 59.2% to 80.5%. In the same duration the number of households that have suffered OOP expenditure on medicines have gone up from 57.5% to 79%.
The study claims that 310 million people have paid out of their own pocket for medicines in the year 2011-12. Out of these, nearly 38 million people were pushed into poverty due to OOP expenditure on medicines.
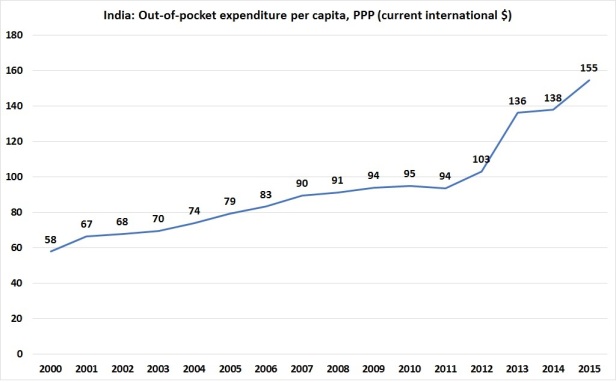
According to an analysis of the World Bank data, in the past 15 years the out of pocket expenditure per capita in India has increased by a whooping 167%. The OOP expenditure per capita, PPP ($) in the year 2000 was $ 58 which went up to $ 155 in the year 2015.
The authors of the BMJ study argue that the reason why Indians are spending more on medicines and falling into poverty is because the OOP expenditure on medicines in India is more than the expenditure on hospitalization or beds which are often subsidized by the government. Other reasons, according to the authors, are under spending on medicines by state governments, inefficient drug procurement and supply chain system thus leading to shortage of medicines in public health facilities and affordability of medicines.
Due to inadequate availability of medicines in public health facilities, people start buying medicines from private facilities, thus increasing the overall cost significantly. The study endorses the central procurement and supply-chain mechanism of Tamil Nadu ans Rajasthan.
